DOCTORAL THESIS | HARVARD T.H. CHAN SCHOOL OF PUBLIC HEALTH | 2026 Naming
the Wound.
Rewriting
the Record.

Why is women’s fibroid suffering not recognised as a measurable burden or a policy concern?
This mixed methods study examines how health system design produces and sustains fibroid invisibility, and what that exclusion costs women, households and the health system.
What this is.
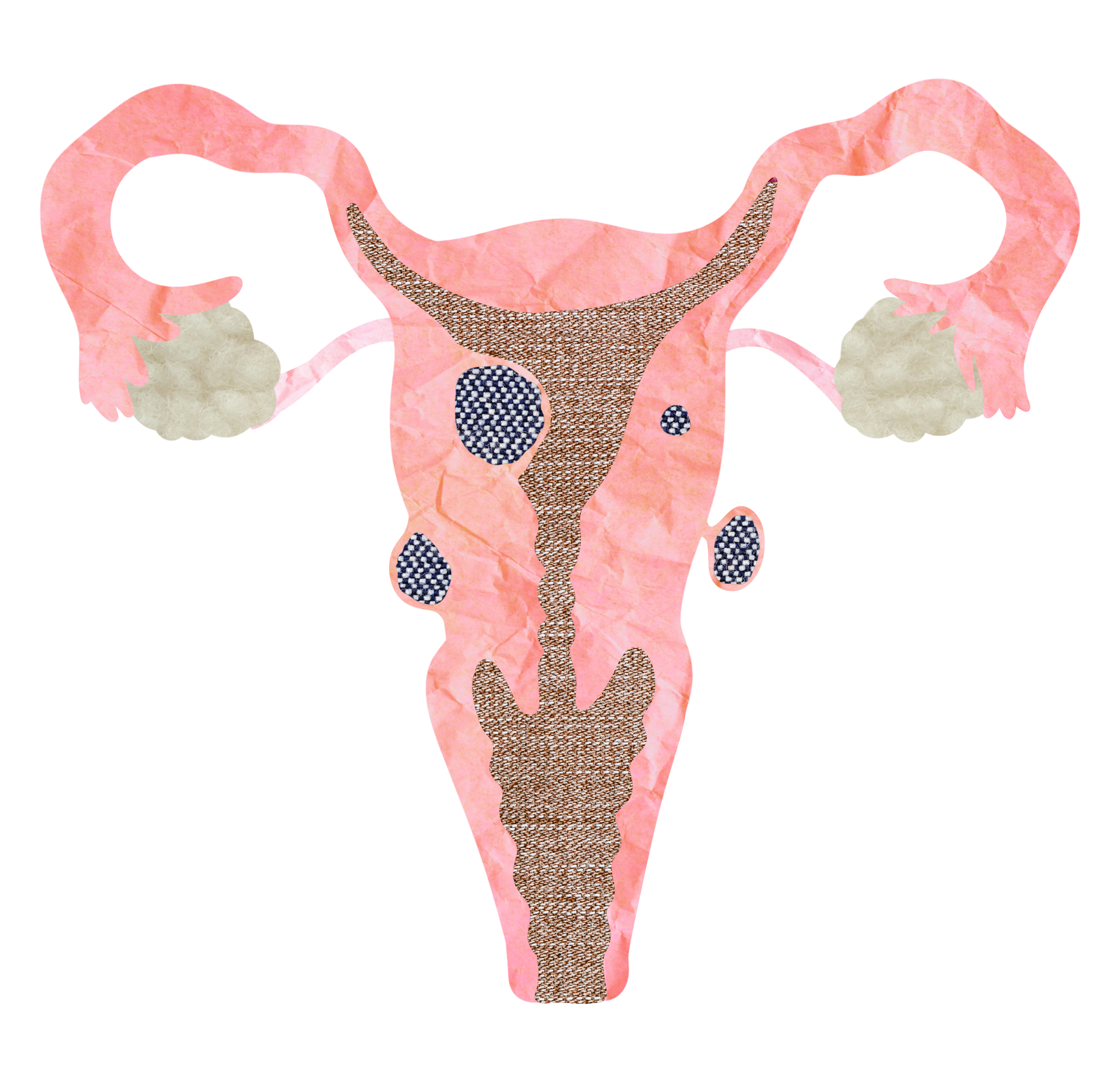
Uterine fibroids are common growths made of muscle and fibrous tissue that develop in or around the uterus. They are noncancerous. Many cause no symptoms. Others can cause heavy or prolonged bleeding, anaemia, pelvic pain or pressure, abdominal swelling, bladder or bowel symptoms, difficulty becoming or remaining pregnant and complications during pregnancy. The impact depends on the number, size and location of the fibroids.
Fibroids occur across populations. In a United States ultrasound study, estimated cumulative incidence by age 50 exceeded 80 percent among Black women and approached 70 percent among white women. Evidence generated on the African continent remains limited. A population based study in central Nigeria found fibroids by transvaginal ultrasound in 45.1 percent of 486 women, while only 7.2 percent reported a prior diagnosis from a health professional. No population based estimate for Sierra Leone was identified in the evidence reviewed for this work.
Care may include monitoring, treatment of bleeding and anaemia, medicines, minimally invasive procedures, myomectomy or hysterectomy. The appropriate pathway depends on symptoms, clinical findings, fertility goals and the woman’s preferences.
Fibroids are noncancerous. Their consequences can still reach into blood loss, fertility, income, work, recovery and peace of mind.
-
Source: Wurie, 2026, Chapter 2, pp. 11 to 12. THESIS BIBLIOGRAPHY: Stewart et al., 2016; Baird et al., 2003.
Source: Morhason-Bello and Adebamowo, 2022 is cited in the thesis text but is absent from the final thesis bibliography.
Source: Adebamowo et al., 2023, Scientific Reports 13:9091. This central Nigerian cohort evidence was reviewed after thesis submission.
The question this thesis examines is not whether treatment is possible. It is whether women can reach it.
A note on the language
The clinical literature calls these growths benign. The clinical term benign means noncancerous. In ordinary language, however, it can be heard as harmless. Fibroids reveal the distance between those meanings. Ask the women in this thesis whether five years of bleeding, anaemia, infertility, surgery costing a year's income, and being called cursed by a mother-in-law for childlessness she did not choose is harmless. The vocabulary is part of what this work corrects. The same applies to heavy bleeding, discomfort, and common. Words that minimise are not neutral. They are how administrative invisibility is held in place.
A Letter from the AuthorThe silence was the finding.
The silence did not remain empty. It appeared in missing data, absent financing, delayed diagnosis, limited explanation, household debt, moral judgement and survival labour.
Across global health systems, some forms of women's suffering receive policy attention and financing. Others are absorbed into silence. This thesis begins in that silence. It examines how uterine fibroids, a condition affecting up to eighty percent of women of African descent and one in three women seeking gynaecologic care at Sierra Leone's largest referral hospital, remain largely uncounted and unprioritised within the systems responsible for women's health.
The central question is not why women suffer. It is why their suffering is not recognised as a measurable burden or a policy concern. Fibroids appear in no national policy document in Sierra Leone. They are absent from the Health Management Information System. They are not covered under the Free Health Care Initiative, which since 2010 has supported services for pregnant women, lactating mothers, and children under five. There is no allocation for diagnostics, medications, surgery, or reimbursement for fibroid-related care.
In 2025, I sat with women at Princess Christian Maternity Hospital who had been bleeding for years, sold sewing machines to pay for surgery, and been called cursed by their mothers-in-law for infertility they did not know was caused by tumours pressing against their uteruses. I sat with clinicians who diagnose by hand because the ultrasound is broken or locked in the maternity ward. I read 262 charts. I followed the data into kitchens and prayer rooms and trading stalls. I followed it into my own body, too. I do not pretend distance I did not have.
The burden documented here emerges from pathology. Its persistence emerges from policy.
What this research reveals is that fibroid invisibility is not the residue of scarce resources or cultural reluctance. It is the outcome of design. Metrics follow money. Money follows mortality. When health systems are built to count maternal deaths and not chronic gynaecologic morbidity, women's pain becomes administratively invisible, and administrative invisibility produces material suffering. The Free Health Care Initiative is proof that Sierra Leone can mobilise around a defined priority. The exclusion of fibroids is proof that the priority has been narrowly defined.
I dedicate this work to my daughter Amanah Seray, whose name means trust. To be entrusted is sacred. I hope to live in a world that listens when women speak, believes their pain, honours their knowledge, and invests in their healing. Until then, this is the record.
Methodology as PoliticsWhat counts as evidence.
The literature review established what was known and where the record remained thin. The fieldwork generated an explanation from Sierra Leonean data. Hospital records, women’s accounts, family and provider perspectives, policy documents and community knowledge were read together.
I began with women. With twenty-seven women in Freetown, Lumley, Brookfields, Mountain Cut, Kissy, and Waterloo. With their accounts of bleeding and silence and survival. With what they had learned about their own bodies in the absence of clinical explanation. Their testimony is the primary data source of this thesis. It is not anecdote. It is not colour. It is the archive that the formal record has refused to maintain.
The methodological choice is also a political one. Grounded theory holds that categories must emerge from data rather than be imposed upon it. In a context where the data systems themselves are the instrument of erasure, this is not a procedural preference. It is a stance. The Cycle of Suffering and Resilience did not exist before these women spoke. It exists because they did.
Source: THESIS: Wurie, 2026, Chapters 1, 3 and 5, pp. 1 to 9, 21 to 35 and 53 to 64.
PRINCIPLE · 01Narratives are infrastructure
Women's accounts reveal how institutions function, not only how individuals experience them. The story of one woman selling her sewing machine to pay for surgery is a story about categorical health financing. Each testimony documents an architecture.
PRINCIPLE · 02Health systems are not neutral
Indicators, eligibility lines, procurement codes, and reporting templates encode priorities. They are choices, not natural arrangements. The exclusion of chronic gynaecologic conditions from national reporting is not an oversight. It is a definition of whose suffering counts.
PRINCIPLE · 03Resilience is an indictment
Women's labour through illness, household resource mobilisation, and continued caregiving sustain systems that fail them. To celebrate resilience without naming what produced it is to launder structural violence as cultural virtue. The framework refuses this.
Study Design at a GlanceThe rigour beneath the record.
A convergent mixed methods design, traceable from primary data to a framework developed through the dissertation. Every figure on this site is anchored here.
Three Women, NamedThe data has shape.
The shape has lives.
Three case histories from the thesis. Names changed. Geographies kept. Each story illustrates a stage of the cycle that would later be named COSAR. Each life precedes the framework.
Mariama
Age 32 at first symptom · Five years to surgeryAt thirty-two, Mariama noticed unusually heavy bleeding. Over the next three years she presented at four facilities. At each, providers offered iron tablets, pain medication, herbal preparations. No one ordered imaging. By year five, when her abdomen visibly enlarged, she finally received an ultrasound at a private facility her family had financed through collective savings. Surgery cost Le 4.5 million, more than her annual income from market selling. The family mobilised resources for eight months before she could afford the procedure.
What this revealsClinical encounters without diagnostic capacity. Five years between the first bleeding and the operation that addressed its cause. Mariama did not delay. The system did.
Aminata
In her husband's words · Six facilities · Weeks of saving
"We took her to Massakah, Makeni, Four Mile, Wilul, Joriop. Nothing worked until PCMH. When we suspect fibroid but cannot confirm without imaging, somebody borrowed a machine for imaging. It cost Le 300,000. We couldn't afford. So we saved for weeks."
What this revealsThe geography of diagnostic delay. Five facilities. A borrowed machine. Weeks of saving for a single scan. The labour of finding the diagnosis, before the labour of paying for the treatment.
Hawa
Rural presentation · Referral never converted to a journeyHawa presented at a rural hospital. The provider, when asked about referral to the national centre, explained simply: "We refer to PCMH, but transport is expensive. Some never come back."
What this revealsInvisibility through attrition. The women who do not appear in PCMH data because the referral never converted to a journey. The provider knows. The system records nothing.
The WitnessesWomen’s testimony. The first record.
Fifteen in-depth interviews. Five focus group discussions. Seven key informant interviews. The voices below are a fragment of what was shared, set down here with permission, with care, and without translation (Krio material was transcribed in Krio and translated into English with attention to conceptual meaning and idiom).
VC · 41 · Lumley"I sold my sewing machine and my phone to pay for surgery. After the operation, I had nothing left to restart my business."
On Financial Exclusion
VC · 28 · Brookfields"The doctor said I have fibroid. I asked what causes it. He said, "It just happens." That was all."
On Clinical Disregard
VC · 31 · Waterloo
"My mother-in-law said I am cursed, that God is punishing me for something I did."
On Moral Surveillance
VC · 33 · Brookfields"When the hospital did not explain, I asked my mother. She said it is from not having children early."
On Epistemic Negotiation
VC · 41 · Kissy"I went to clinic many times. They gave me iron tablets. Nobody told me fibroid until I reach PCMH. "
On Diagnostic Invisibility
VC · 39 · Lumley"If I don't sell, my children don't eat."
On Survival Labour
What makes the study distinctive
To the best of my knowledge, this is the first known systematic mixed methods study of uterine fibroid invisibility in Sierra Leone and part of a small African mixed methods evidence base. Its originality lies in what it brings together: the national referral record, women’s accounts, family and provider perspectives, traditional and community knowledge, household economics, policy design and health information systems. COSAR emerged from that integration.
Visible limitations
This study reviewed admissions at one national tertiary hospital during a six week period. The 34% figure describes the proportion of admissions reviewed at PCMH. It does not estimate national prevalence.
The qualitative sample was purposive and concentrated in Freetown and peri urban Western Area. It was designed for depth, variation and explanation. Rural experiences require direct study. The design was cross sectional and some participant accounts relied on recall. Translation from Krio into English also required interpretive judgement.
These limits define the scope of the findings and point directly to the next research study.
Source: Wurie, 2026, Study Limitations, pp. 38 to 40 and 73 to 74.
Every gynaecological admission recorded at PCMH during the study window was reviewed.
Women’s accounts were analysed as evidence and generated the explanatory categories.
Clinical, social, economic and policy evidence were analysed together.
COSAR emerged as an original Sierra Leonean framework with six interacting mechanisms.
The study identifies reform points across data, financing, diagnosis, communication, social protection and recovery.
The FindingsWhat the data refuses to hide.
A retrospective chart review of 262 gynaecological admissions at Sierra Leone's national referral hospital, paired with twenty-seven qualitative voices. Together, they make a record where none existed before. Three numbers carry the weight of the rest.
Clinical Burden34%
Fibroids admissions reviewed at PCMH during the study window.”
The single most common condition women present with at Sierra Leone's national referral hospital. First known systematic mixed methods study of uterine fibroid invisibility in Sierra Leone
Public Coverage0%
Subsidised surgery across 89 cases
No FHCI eligibility. No insurance coverage. Surgical care is entirely out of pocket and costs six to twelve months of median household income.
Anaemia at Admission71%
anaemic when they reached PCMH
Mean haemoglobin 8.3 g/dL. Bleeding sustained over years while women continued their daily labour at home and at market.
34%
Clinical burden
Of gynaecologic admissions at PCMH attributed to fibroids. The single most common condition women present with.
0%
Public coverage
FHCI or insurance subsidy for fibroid surgery across 89 cases. Treatment is entirely out-of-pocket.
62%
Diagnostic delay
Of cases with documented symptom duration delayed more than three months before diagnosis.
38%
Nulliparity
Of women with fibroids were nulliparous. Roughly ten times the national rate.
71%
Anaemic at admission
Reflecting chronic bleeding sustained while women continued daily labour.
96%
No counselling documented
Charts contained no record of risk factors, options, or recovery expectations discussed.
Le 2 to 9M
Surgical cost
The equivalent of six to twelve months of median household income. Asset liquidation, borrowing, prolonged saving.
69 of 89
employed or self employed.
Continued earning through symptoms. No social protection. Household survival depends on women's labour.
From 262 ChartsA national picture, plainly told.
The chart review establishes burden at the tertiary referral hospital. It cannot, on its own, establish national prevalence. What follows is a transparent extrapolation, building from the thesis data and the published literature on uterine fibroids in women of African descent. Every assumption is named. Every number can be checked. This is the first such public estimate for Sierra Leone, and it is offered to make the case that a proper prevalence study is overdue.
What PCMH seesEighty nine cases in six weeks. About seven hundred per year.
The chart review captured 89 confirmed fibroid admissions across six weeks at PCMH. Annualised at the same rate, that is approximately seven hundred women per year reaching the country's tertiary gynaecological hospital with a confirmed diagnosis. Most of them after years of presenting elsewhere without one.
~712
Fibroid admissions at
PCMH per yearThe population at riskRoughly two million reproductive-age women.
Sierra Leone's female population aged 15 to 49 sits at approximately two million (Statistics Sierra Leone, 2021 Population and Housing Census; UN World Population Prospects). Women of African descent carry the highest documented lifetime fibroid risk in the published literature: up to eighty per cent by age fifty (Baird et al., 2003; Marsh et al., 2013). These two facts have never, until now, been placed beside Sierra Leone hospital data.
~2.0M
Women aged 15 to 49 in Sierra LeoneThis study establishes a serious signal within national referral care and explains how women become invisible before reaching it. It does not tell us how many women in Sierra Leone have fibroids.
Sierra Leone now needs a nationally representative, ultrasound confirmed study across urban and rural settings, linked to symptoms, prior diagnosis, anaemia, management access, household cost and facility readiness.
-
Source: Wurie, 2026, Study Limitations and Future Investigation, pp. 38 to 40 and 85 to 86.
Source: Morhason-Bello and Adebamowo, 2022 is cited in the thesis text but missing from the final bibliography.
Source: Adebamowo et al., 2023, Scientific Reports 13:9091 and 13:18926. These studies support ultrasound confirmation and show why diagnosed cases cannot provide a population denominator.
Assumptions named
The PCMH annualisation assumes the six week study window is representative of the year. The 80% lifetime figure is drawn from US studies of women of African descent (Baird et al., 2003) and may differ for West African populations specifically; no published Sierra Leone or West Africa prevalence study currently exists. The 20% to 30% symptomatic range is conservative and drawn from clinical reviews. Sierra Leone female population figures use Statistics Sierra Leone 2021 Census projections and UN World Population Prospects estimates. This extrapolation is offered as a transparent public estimate, not a peer reviewed prevalence study. It is the first of its kind for Sierra Leone, and it is offered precisely to make the case that one is needed.
An Original FrameworkThe Cycle of Suffering and Resilience.
COSAR did not precede the data. It emerged from it, through systematic engagement with 89 clinical cases and 27 voices in Sierra Leone. Six interconnected mechanisms by which system-level design produces lived experience, and through which individual adaptation absorbs system failure, allowing the gaps to persist.
Diagnostic
Invisibility

Survival
Labour
1
6
Moral
Surveillance
Clinical
Disregard
2
COSAR
CYCLE OF SUFFERING
AND RESILIENCE
F. WURIE · 2026
5
3
4
Epistemic
Negotiation
Financial
Exclusion
Reading COSAR analyticallyCOSAR shows where the care pathway breaks and where reform can begin.
Source: THESIS: Wurie, 2026, Integrated Findings and Discussion, pp. 43 to 64.
Fibroid care should begin before the operating theatre. Women in this study often reached PCMH after repeated presentations, unaffordable imaging and prolonged symptoms. By that stage, surgery was often the dominant recorded option. Women unable to finance it remained in the cycle.
COSAR shows where the pathway breaks: recognition, diagnosis, explanation, financing, social protection and recovery. It explains how care narrows toward the most invasive endpoint when earlier management remains unavailable or unaffordable.
What the Sierra Leone data showsCOSAR mechanism naming the breakStandard management stageFourteen of the fifteen women interviewed reported no prior awareness before diagnosis. Most presented after years of bleeding, pain, or infertility had escalated.
01 · Diagnostic Invisibility
Early symptom recognition
13.5% had ultrasound before admission. 42% diagnosed by clinical examination alone. 62% experienced delays of more than three months.
01 · Diagnostic Invisibility
Diagnostic imaging
96% no counselling documented. No record of risk factors, treatment alternatives, or recovery expectations discussed.
02 · Clinical Disregard
Counselling and explanation of options
-
WHAT THE SIERRA LEONE DATA SHOWS:
Fourteen of the fifteen women interviewed reported no prior awareness before diagnosis. Most presented after years of bleeding, pain, or infertility had escalated.
COSAR MECHANISM NAMING THE BREAK:
01 · Diagnostic Invisibility
-
WHAT THE SIERRA LEONE DATA SHOWS:
13.5% had ultrasound before admission. 42% diagnosed by clinical examination alone. 62% experienced delays of more than three months.
COSAR MECHANISM NAMING THE BREAK:
01 · Diagnostic Invisibility
-
WHAT THE SIERRA LEONE DATA SHOWS:
96% no counselling documented. No record of risk factors, treatment alternatives, or recovery expectations discussed.
COSAR MECHANISM NAMING THE BREAK:
02 · Clinical Disregard
-
WHAT THE SIERRA LEONE DATA SHOWS:
0% received written materials. Women constructed understanding from mothers, friends, church members, and traditional healers in the absence of clinical explanation.
COSAR MECHANISM NAMING THE BREAK:
03 · Epistemic Negotiation
-
WHAT THE SIERRA LEONE DATA SHOWS:
No FHCI coverage. Effectively out of reach for households without private resources. Anaemia (71% at admission) was managed through endurance rather than intervention.
COSAR MECHANISM NAMING THE BREAK:
04 · Financial Exclusion
-
WHAT THE SIERRA LEONE DATA SHOWS:
Where it occurred, it was the absence of intervention by default, not by clinical decision. Women returned to the system only when the disease had progressed.
COSAR MECHANISM NAMING THE BREAK:
01 + 04 · Invisibility, Exclusion
-
WHAT THE SIERRA LEONE DATA SHOWS:
Unavailable in the public system. Concentrated in private and overseas facilities, financially inaccessible for most households.
COSAR MECHANISM NAMING THE BREAK:
04 · Financial Exclusion
-
WHAT THE SIERRA LEONE DATA SHOWS:
The dominant clinical encounter. 0% public coverage. Le 2 to 9 million per case at PCMH, the government tertiary hospital, paid entirely by the household.
COSAR MECHANISM NAMING THE BREAK:
04 · Financial Exclusion
-
WHAT THE SIERRA LEONE DATA SHOWS:
38.2% nulliparous (ten times the national rate). One third presented with infertility. Childlessness moralised as personal or spiritual failing.
COSAR MECHANISM NAMING THE BREAK:
05 · Moral Surveillance
-
WHAT THE SIERRA LEONE DATA SHOWS:
77.5% economically active despite chronic symptoms. Women returned to market trading or farming days after surgery because no social protection or sick leave exists.
COSAR MECHANISM NAMING THE BREAK:
06 · Survival Labour
0% received written materials. Women constructed understanding from mothers, friends, church members, and traditional healers in the absence of clinical explanation.
03 · Epistemic Negotiation
Patient education and written materials
No FHCI coverage. Effectively out of reach for households without private resources. Anaemia (71% at admission) was managed through endurance rather than intervention.
04 · Financial Exclusion
Medical management (hormonal therapy, iron, tranexamic acid)
Where it occurred, it was the absence of intervention by default, not by clinical decision. Women returned to the system only when the disease had progressed.
01 + 04 · Invisibility, Exclusion
Watchful waiting with active monitoring
Unavailable in the public system. Concentrated in private and overseas facilities, financially inaccessible for most households.
04 · Financial Exclusion
Interventional options (arterial embolisation, hormonal IUD)
The dominant clinical encounter. 0% public coverage. Le 2 to 9 million per case at PCMH, the government tertiary hospital, paid entirely by the household.
04 · Financial Exclusion
Surgical management
38.2% nulliparous (ten times the national rate). One third presented with infertility. Childlessness moralised as personal or spiritual failing.
05 · Moral Surveillance
Support for childlessness and social impact
77.5% economically active despite chronic symptoms. Women returned to market trading or farming days after surgery because no social protection or sick leave exists.
06 · Survival Labour
Post-operative recovery and return to function
The management pathway exists. It exists in clinical guidelines and in the practice of every health system that has taken women's chronic gynaecological burden seriously.
It does not exist in operational form for women in Sierra Leone.
COSAR is the diagnostic of that absence. Each mechanism is the name of an intervention that should have happened and did not. Reform that targets only the surgical endpoint without addressing every earlier stage will produce the same outcome at a higher cost. The whole pathway is the management piece. COSAR is how it is read.

01
Diagnostic Invisibility
62% delayed > 3 months
42% diagnosed by clinical exam alone
13.5% had an ultrasound before admission
Equipment is concentrated in antenatal services. Imaging requires private payment. Providers adapt to scarcity by managing symptoms while waiting for the tumour to become palpable. Diagnosis is not a question of clinical skill. It is a question of access to the machine.
02
Clinical Disregard
Counselling was documented in four of 89 records.
40 to 50 patients per clinic session
~5 minutes per consultation
This is not provider failure. It is throughput. When a single gynaecologist must move forty women through a morning, communication contracts to the diagnostic noun and the surgical recommendation. Women receive verdicts. Not explanations.
03
Epistemic Negotiation
97% no prior fibroid awareness
0% received written materials
Knowledge constructed from mothers, friends, faith
Where biomedical systems provide diagnosis without explanation, women construct understanding from the materials available. Family knowledge. Church members. Traditional healers. The vacuum produced by the clinic gets filled by the community. This is not superstition. It is pragmatism.
04
Financial Exclusion
Le 2 to 9M surgical costs
0% FHCI coverage
Six to twelve months household income
The FHCI covers pregnancy. It does not cover fibroids. The same woman who delivers her child at state expense will pay privately if her uterus bleeds her into anaemia six months later. Categorical financing is not a budget constraint. It is a definition of which women count.
05
Moral Surveillance
38% nulliparous (10× national rate)
33% presented with infertility
Childlessness moralised in absence of explanation
Diagnostic delay produces temporal space. In that space, fibroid-related infertility is interpreted as curse, as punishment, as personal moral failure. The biomedical system's silence becomes a community's licence to judge. The body's tumour becomes the woman's shame.
06
Survival Labour
77.5% economically active through symptoms
71% anaemic at admission
No social protection for chronic illness
Women keep selling. They keep cooking. They keep their children fed. Resilience here is not virtue. It is the absence of any alternative. To call this adaptation "strength" without naming what produced it is to launder structural violence as cultural character.
The Cycle of Suffering and Resilience was developed by Fatou Wurie through doctoral fieldwork at Princess Christian Maternity Hospital, Freetown, between January and August 2025. It is the conceptual contribution of this thesis. Researchers, clinicians, and policymakers are welcome to test its six mechanisms against other neglected reproductive conditions and other contexts. The framework is open. Attribution is required.
An original framework developed through this doctoral research.
Wurie, F. (2026). Naming the Wound, Rewriting the Record: Uterine Fibroids and the Cost of Silence in Sierra Leone. Doctoral thesis, Harvard T.H. Chan School of Public Health. COSAR framework, original.

Sierra Leone & The Continental FrameThe country has shown what is possible.
Over a decade and a half, Sierra Leone built one of the most ambitious maternal health architectures on the African continent. Maternal mortality fell from roughly 1,160 per 100,000 live births in 2019 to 354 in 2023. The infrastructure proves capacity. The exclusion of chronic gynaecologic conditions proves that the priority has been narrowly defined. COSAR documents what that exclusion produces.

The argument in one paragraph.
The Free Health Care Initiative, launched in 2010, demonstrated that the state could remove user fees and move women into facilities for delivery. Sixteen years of investment followed: more than 4,000 health workers recruited, 1,600 facilities rehabilitated, 300+ solarised, 12 oxygen plants installed, a National Emergency Medical Service built, a maternal digital registry enrolling more than 400,000 pregnancies, a Climate-Health Unit established in 2024, and the 300 Days of Activism for Triple Zero launched by President Bio on 2 March 2026.
Sierra Leone has already shown what becomes possible when women’s health is made a national priority. The next choice is to extend that ambition beyond pregnancy. The capacity is in place. The architecture exists. What is missing is the categorical decision to extend it across the full arc of women's reproductive lives.
A National Architecture · 2010 to 2026
Across The ContinentThe financing question.
Sierra Leone's health expenditure is split across three sources. Government contributes between 14 and 17 per cent. Development partners contribute between 34 and 36 per cent. Households carry 52 per cent through out-of-pocket payments. For women with fibroids, that 52 per cent is 100 per cent. There is no public protection. There is no donor category. There is no insurance line. The full cost of care comes from her household, or it does not come at all. This is the arithmetic of categorical exclusion.
Households · out-of-pocket
52%
Where fibroid care lives. 100% out-of-pocket for women excluded from FHCI.
Development partners
34 to 36%
Under documented retrenchment. The Lusaka Agenda anchors the domestic transition.
Government of Sierra Leone
14 to 17%
Health allocation at 11–12% of national budget. Moving toward Abuja target of 15%.
"Metrics follow money. Money follows mortality. Until reproductive morbidity is measured with the same investment and urgency as maternal mortality, the aspiration of healthy and empowered women will remain constrained."
Chapter 1, Naming the Wound, Rewriting the Record
RecommendationsEight policy opportunities. One highest leverage move.
The thesis closes with eight specific recommendations grouped at three altitudes: national reforms for Sierra Leone, health system operational changes, and continental policy positioning. They are designed to be sequenced, not selected from. The single highest leverage starting point is named first.

The Highest Leverage InterventionIntegrate chronic gynaecological conditions into DHIS2.
Of the eight recommendations, this one is named first because it conditions the rest. DHIS2 integration is the most achievable starting point. It requires software configuration rather than political battles over budgets or workforce expansion. Once fibroids and other chronic gynaecological conditions appear in district dashboards, visibility creates accountability. Accountability creates measurement. Measurement precedes financing. The eight recommendations downstream all become more feasible the moment chronic gynaecological burden is visible in the national health information system.
Eight policy opportunities. One highest leverage move.
RECOMMENDATION 01
Expand FHCI eligibility to chronic gynaecological conditions
Move from pregnancy specific to condition neutral reproductive health coverage. Phase 1 (Years 1 to 2): surgical management of symptomatic fibroids and gynaecological cancers. Phase 2 (Years 3 to 5): comprehensive gynaecological care.
Lead: Ministry of Health and Sanitation with Treasury. Partners: development agencies currently supporting FHCI.
RECOMMENDATION 02
Integrate chronic gynaecological conditions into DHIS2
Build a gynaecological module parallel to the existing maternal health modules. Standardised data fields for gynaecological admis-sions by diagnosis, surgical procedures, imaging utilisation, diagnostic delays, and treatment costs. Twelve month pilot before full rollout.
Lead: DHIS2 technical team with WHO support. Mandated through facility performance contracts.
RECOMMENDATION 03
Establish social protection for chronic illness
Temporary income replacement during medically certified illness, subsidised childcare enabling women to prioritise health, transport vouchers for specialty care access. Pilot through existing National Social Safety Net Programme infrastructure.
Partners: women's cooperatives and market associations for identification and distribution.
Health System Operations
RECOMMENDATION 04
Redistribute diagnostic equipment to gynaecological services
Current ultrasound capacity concentrates in antenatal clinics. Reallocate to ensure each district and tertiary gynaecological service point has functional imaging with active maintenance contracts. One functional ultrasound per gynaecological service point as the floor.
Lead: Ministry of Health and Sanitation with WHO and UNFPA support.
RECOMMENDATION 05
Expand the gynaecology workforce, lower patient provider ratios
Current ratios of forty to fifty patients per session preclude adequate consultation. Accelerated mid level provider training. Task shifting of examination and counselling to trained nurses. Public sector incentive packages for specialists. Target: fifteen to twenty patients per session within three years.
Partners: Global Fund and GAVI for workforce financing tied to FHCI extension.
RECOMMENDATION 06
Develop patient education materials and counselling protocols
Multilingual written materials in English, Krio, Mende, and Temne. Visual aids explaining uterine anatomy and fibroid development. Treatment option comparison tools. Standardised counselling protocols. Pilot at PCMH in collaboration with FIGO and UNFPA, then scale through the Ministry's Reproductive Health Division.
Lead: PCMH gynaecology department. Partners: FIGO, UNFPA, MoHS RHD.
Continental Frameworks
RECOMMENDATION 07
Position chronic gynaecological conditions in Agenda 2063 and the Maputo Plan of Action
Integrate indicators and commitments for fibroid care access, gynaecological cancer screening, endometriosis management, and comprehensive uterine health into the next Maputo Plan review. Continental frameworks shape national priorities; visibility there forces accountability across the African Union.
Lead: OAFLAD, FIGO Africa Regional Council, Women in Global Health Africa. Backing: AU Department of Health, WHO Africa, WAHO.
RECOMMENDATION 08
Support regional centres of excellence for uterine health
Establish regional training and research hubs advancing uterine health diagnosis and care across West Africa. Cross country research partnerships. Harmonised clinical protocols. Comparative population studies that the Sierra Leone case has shown to be urgent.
Partners: WAHO, FIGO Africa, regional academic institutions, OAFLAD First Ladies network.
Across The ContinentThe cycle is not unique to Sierra Leone.
COSAR was built around fibroids in Sierra Leone, but the pattern it documents recurs across African and diasporic contexts. Different health systems. Same architecture of exclusion. The data below is drawn from the thesis literature review.
KENYA
68%
Of women delayed seeking care for fibroid symptoms by more than one year. Cited shame and fear of bewitchment as primary reasons.
GICHUHI ET AL., 2021
NIGERIA
30%
Of national gynaecologic admissions attributed to fibroids. Diagnostic delays of one to three years normalised as "ordinary female problems."
FMOH UTERINE HEALTH ROUNDTABLE, 2025
SOUTH AFRICA
Racial gap
Black women face longer diagnostic delays and higher surgical costs than white women. Race compounds gendered neglect within the same national system.
WISE ET AL., 2020
USA & UK
2-3×
Black women more likely than white women to undergo hysterectomy for fibroids. Receive a fraction of the research investment of comparable male reproductive disorders.
STEWART ET AL., 2017
GLOBALLY
< 1%
Of annual global health funding targets non-maternal gynaecologic morbidity. What threatens fertility or life commands resources. What diminishes daily living does not.
IHME, 2023
The mechanisms operate similarly across both low-income and high-income contexts. The same hierarchy of visibility is reproduced wherever reproductive health frameworks are organised around maternity. COSAR offers an analytical framework potentially applicable across the continent and beyond.
From Evidence to PracticeYouterus is the practical translation of this work.
Youterus Health is Africa's uterine health company. Headquartered in Freetown, with operations in Nigeria and Kenya, Youterus translates the diagnosis at the heart of this thesis into infrastructure: data, financing, clinical pathways, and policy advocacy. COSAR is the analytical foundation. Youterus is the response.
I entered the doctorate knowing I wanted to build. The research gave me the evidence and language to define the institution more clearly. Listening to women, clinicians, healers and families revealed four gaps: community recognition, reliable referral, financial protection and data. I founded Youterus Health around those gaps.
COSAR gave a systems language to what women described. It showed how gaps reinforce one another and where the care pathway breaks. Together with sustained listening, COSAR informed the development of our WOMB Index, a community level uterine health risk identification and referral tool designed for settings where imaging is scarce.
The doctoral study was conducted and analysed independently of Youterus Health programmes. The research, COSAR, the WOMB Index and Youterus share an intellectual lineage because they grew from the same body of listening and analysis.
Source: Wurie, 2026, independence statement, p. 10. LEADERSHIP REFLECTION: From Research to Institution and Narrative as Evidence, pp. 15 to 16 and 21 to 26. A public validation or first claim for the WOMB Index requires its own verifiable source.
PILLAR · 01
The WOMB Index
An eight-dimension instrument for documenting uterine health burden, validated against SAMANTA, and currently deployed across six districts in Sierra Leone with 1,000 women in its Phase 1 cohort.
PILLAR · 02
The Unmute the Womb Programme
A multi-country advocacy and clinical pathway programme spanning Sierra Leone and Nigeria, supported by the Gates Foundation, in coalition with WRA Nigeria, Qhala, and the AMC Working Group. The campaign that names what has been silent.
PILLAR · 03
The Uterine Health Fund
Direct financing for women whose surgeries fall outside FHCI. Eighty-plus myomectomies and hysterectomies funded to date. Until the state expands coverage, women cannot wait. The fund is the bridge.
PILLAR · 04
UTERO
An AI-enabled uterine health intelligence platform built atop the WOMB Data Registry. A dedicated data platform for chronic gynaecological conditions. Visibility, at scale.
The JourneyOn doctorate, leadership, and motherhood. This thesis carries three inheritances.
What Comes NextThe framework opens questions.
COSAR was built around fibroids in Sierra Leone, but its mechanisms may illuminate dynamics far beyond that context. The thesis closes by opening four lines of further investigation. They are offered here as invitations to other researchers, clinicians, and policymakers carrying this work forward.
-
The framework emerged from fibroids in Sierra Leone, but its six mechanisms may illuminate dynamics affecting endometriosis, adenomyosis, pelvic inflammatory disease, and gynaecologic cancers across contexts that share similar structural conditions. The question is empirical and open.
-
COSAR suggests that interventions targeting multiple cycle stages simultaneously achieve greater impact than reforms addressing single barriers. Testing this hypothesis requires implementation research comparing different intervention strategies. The case for sequencing matters.
-
Investigation of policymaking processes in contexts where HMIS lacks chronic condition data would illuminate how invisibility shapes priority setting, budget allocation, and which conditions cross the threshold from administrative obscurity into national investment.
-
Comparative analysis of countries that expanded maternal health financing to include chronic gynaecologic conditions would identify successful reform pathways, implementation challenges, and enabling political conditions. The comparison is the policy lesson.
In CoalitionThis work was held by many.
A doctoral thesis appears under a single name. It is never the work of one person. The committee that guided it and the family that carried it deserve to be named first and given their full weight. The wider coalition follows. The thesis itself contains the fuller list.
First, The Doctoral CommitteeThe three who shaped how this work could be done.
They believed the question was worth asking, sat with the evidence as it took shape, and pressed for the rigour that this thesis now carries into the world.
What these three scholars gave the work was deeper than their titles describe. They asked harder questions than the methods chapter required. They held me to the seriousness of what women face when health systems do not respond, and they kept the research honest about what it could and could not say. Their support was not technical guidance bolted onto a doctoral project. It was the long, patient discipline of keeping a study centered on women and refusing the easier framings the field would have allowed. They trusted me to sit with the harder ones.



And The FamilyThe people whose lives made this possible.
A doctoral thesis is years of carried weight. These are the people who carried it with me, often without recognition, and to whom this work belongs alongside the women whose stories sit at its centre.
Website & Creative and Tour AcknowledgementsTo women who helped this work enter the world
The visual language of this thesis journey was shaped by Egle Petkeviciute, Creative Campaigns Lead at Youterus Health.
Egle designed the doctoral defence deck and led the creative development of this website, translating a substantial body of scholarship into a public experience with clarity, feeling and dignity. She contributed her creative direction and design work pro bono, as a gift to the women whose knowledge and stories made this research possible.
The thesis tour was organised by my Aunty Safi. Her planning, coordination, relationship building and care carried the work into each room and made every gathering possible. Isata Kamara, our visual storyteller and photographer, has documented the journey and helped preserve its people, atmosphere and meaning.
With profound gratitude to all three for helping this research enter the world with beauty, discipline and heart.

To every woman still bleeding unseen or unheard: this work is written in witness to you. May it stand as one step in rewriting the record of your lives, your pain, and your power.
EngageRead it. Cite it. Carry it forward.
This thesis was written to be returned to women, to clinicians, to policymakers, to the funders who can move resources, and to the next generation of researchers who will carry it further than I can. The work is open. The framework is mine. The invitation is direct.
01 · ARCHIVE
Read the thesis
The full one hundred and seven pages: chart review, qualitative analysis, the COSAR framework, policy recommendations, and the recommended reforms for Sierra Leone and the wider continent. Now available through Harvard DASH
02 · LEADERSHIP
Read the leadership reflection
The companion document to the doctoral thesis. A reflection on what it took to lead this work from a research question into institutional practice, written for the DrPH leadership portfolio and offered here as part of the public record.
03 · FRAMEWORK
Cite COSAR
The Cycle of Suffering and Resilience is an original analytical framework, developed through doctoral fieldwork in Freetown, 2025. Researchers and policymakers are welcome to test its six mechanisms in other contexts. Attribution is required.
04 · RESEARCH
Build the national evidence
Sierra Leone needs a nationally representative, ultrasound confirmed estimate of fibroid prevalence, linked to symptoms, prior diagnosis, anaemia, management access, household cost and facility readiness.
Feasibility and protocol phase: USD 250,000 to USD 350,000
Full national study: USD 1.3 million to USD 2.2 million
These are indicative planning ranges.
06 · SPEAK
Invitations & press
For speaking, advisory engagements, peer collaboration, and interviews on COSAR, uterine health policy in Africa, or the broader work, please reach out directly.
05 · PARTNER
Work with Youterus Health
Youterus Health partners with ministries of health, multilateral institutions, and aligned funders to integrate uterine health into national priorities across Sierra Leone, Nigeria, and Kenya. The Unmute the Womb coalition is open to new members.
-
A. Primary sources for the website edits
Wurie, F. (2026). Naming the Wound, Rewriting the Record: Uterine Fibroids and the Cost of Silence in Sierra Leone. Doctoral dissertation, Harvard T.H. Chan School of Public Health.
Wurie, F. Leadership Reflection Report. Unpublished working manuscript, Harvard T.H. Chan School of Public Health.
B. References in the thesis bibliography and used in these notes
Baird, D. D., Dunson, D. B., Hill, M. C., Cousins, D. and Schectman, J. M. (2003). High cumulative incidence of uterine leiomyoma in Black and white women: ultrasound evidence. American Journal of Obstetrics and Gynecology, 188(1), 100 to 107. doi:10.1067/mob.2003.99.
Charmaz, K. (2014). Constructing Grounded Theory. Second edition. London: Sage Publications.
Creswell, J. W. and Plano Clark, V. L. (2017). Designing and Conducting Mixed Methods Research. Third edition. Thousand Oaks, CA: Sage.
Government of Sierra Leone. (2010). Free Health Care Initiative Policy Document. Freetown: Government of Sierra Leone.
Kruk, M. E. et al. (2018). High quality health systems in the Sustainable Development Goals era: time for a revolution. The Lancet Global Health, 6(11), e1196 to e1252.
Statistics Sierra Leone and ICF. (2020). Sierra Leone Demographic and Health Survey 2019. Freetown, Sierra Leone, and Rockville, Maryland, USA: Statistics Sierra Leone and ICF. The thesis bibliography lists the survey under 2019; the final report was published in 2020.
Stewart, E. A., Laughlin-Tommaso, S. K., Catherino, W. H., Lalitkumar, S., Gupta, D. and Vollenhoven, B. (2016). Uterine fibroids. Nature Reviews Disease Primers, 2, 16043. doi:10.1038/nrdp.2016.43.
C. Cited in the thesis text but missing from the final thesis bibliography
Morhason-Bello, I. O. and Adebamowo, C. A. (2022). Epidemiology of uterine fibroid in black African women: a systematic scoping review. BMJ Open, 12(8), e052053. doi:10.1136/bmjopen-2021-052053.
D. Additional evidence reviewed after thesis submission
Adebamowo, C. A., Morhason-Bello, I. O., the ACCME Research Group as part of the H3Africa Consortium and Adebamowo, S. N. (2023). Validation of self-report of uterine fibroid diagnosis using a transvaginal ultrasound scan. Scientific Reports, 13, 9091. doi:10.1038/s41598-023-36313-y.
Adebamowo, C. A., the ACCME Research Group as part of the H3Africa Consortium and Adebamowo, S. N. (2023). Population-based study of the reproductive risk factors for transvaginal ultrasound diagnosed uterine fibroids in Nigerian women. Scientific Reports, 13, 18926. doi:10.1038/s41598-023-44703-5.
Akpenpuun, J., Fayehun, O. and Jegede, A. (2019). Health Seeking Behaviour of Tiv Women Living with Fibroid in Benue State, Nigeria. The Nigerian Journal of Sociology and Anthropology, 17(1), 17 to 34. doi:10.36108/NJSA/9102/71(0120).
Fakunmoju, A. J., Fayehun, O. A. and Bello, O. O. (2025). Risk factors for late presentation of symptomatic uterine fibroid in urban Nigeria: a mixed method study. Women’s Health, 21, 17455057251367143. doi:10.1177/17455057251367143.
E. Internal planning document
Wurie, F. (2026). Rewriting the Record: Sierra Leone Fibroid Research Partnership Concept. Internal partnership discussion paper.